What Are Deep-Cheek Sagging and Jowls?
In Korean, the soft tissue that hangs from the corner of the mouth down to the jawline is called "심부볼·불독살·심술보"; the English medical term is jowls. It is tempting to call this "sagging skin," but jowls are not a one-layer problem — they are the visible result of multi-layer aging across bone, deep fat pads, superficial fat pads, the SMAS, and skin. That is why simply "pulling" the area rarely works.
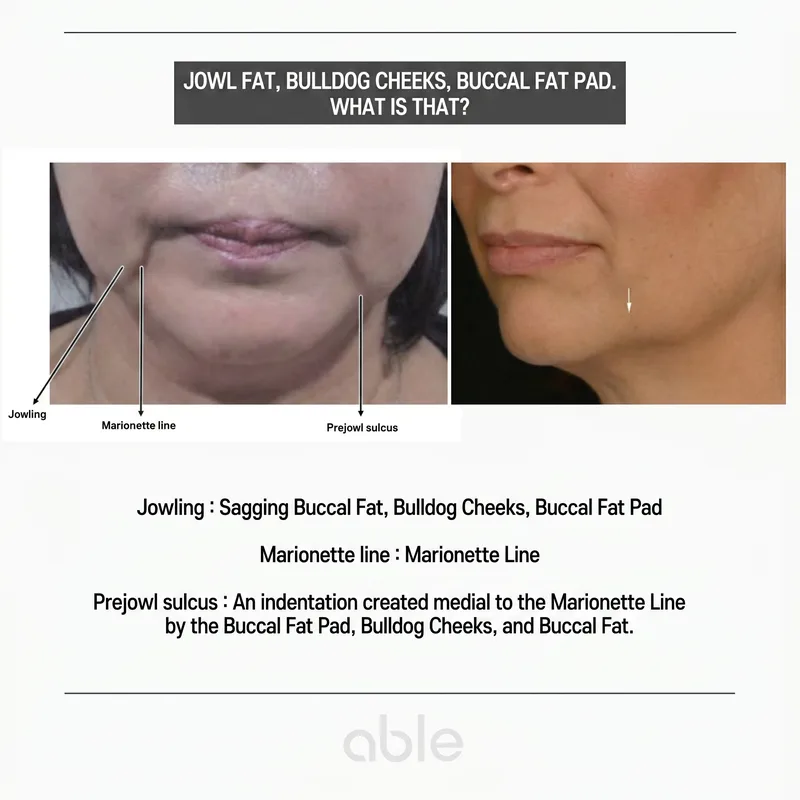
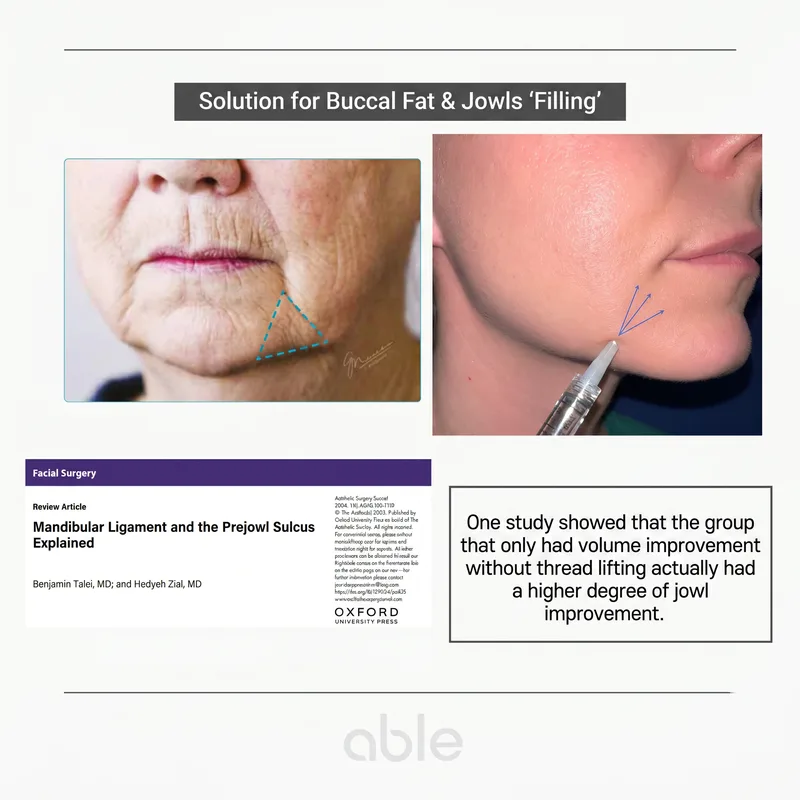
As jowls progress, a shadowed depression forms beside the mouth corner (prejowl sulcus) and the line between mouth corner and chin sags into the marionette line. This area responds poorly to wrinkle-only treatments and requires structural support of the underlying scaffold.
Three Layers That Change Simultaneously with Aging
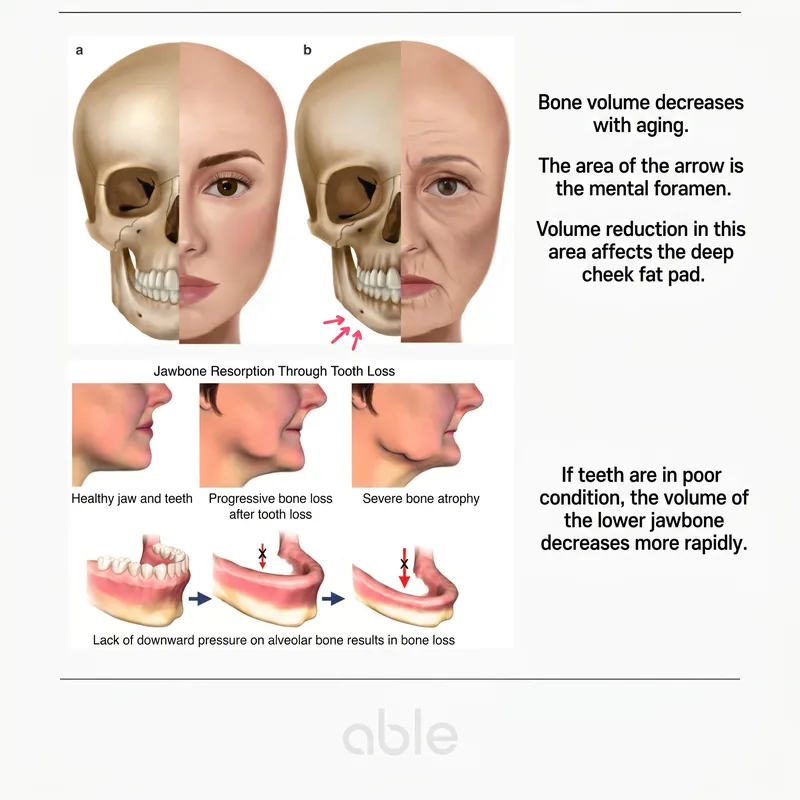
Deep-cheek sagging and jowls reflect simultaneous changes in three distinct layers. ① Bone resorption — the maxilla and mandible resorb progressively with age. Bone loss around the mental foramen and along the anterior mandible directly weakens the support that deep-cheek soft tissue rests on, and dental loss accelerates mandibular bone resorption.
② Atrophy of the deep fat compartments — the deep medial cheek fat and adjacent deep fat pads shrink with age. The result is that the superficial fat above loses its "shelf" and collapses inferomedially.
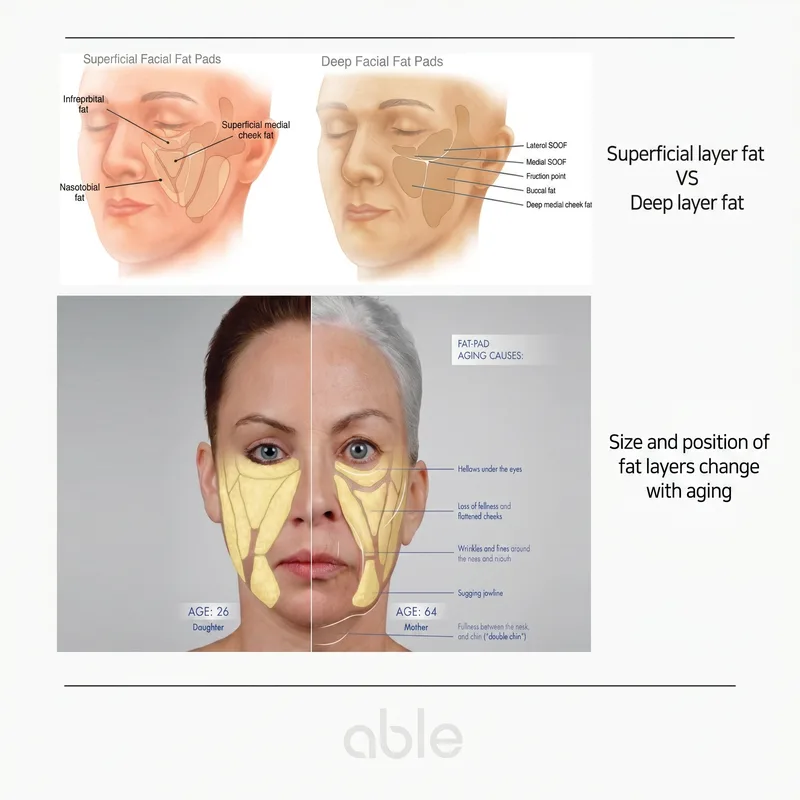
③ Descent of the superficial fat compartments — superficial fat compartments are tethered by retaining ligaments. As those ligaments weaken, the compartments slide inferiorly and create the bunched appearance of jowls at the mandibular border.
"Filling" Beats "Pulling" — The Marionette Filler Approach
Intuitively, sagging tissue suggests "pulling it back up." But without rebuilding the scaffold underneath, surface pulling gives temporary or unnatural results. The key is filling, not pulling. Restoring the lost deep fat and supraperiosteal volume in the right locations rebuilds the shelf, and the superficial fat, SMAS, and skin above settle back into a more natural position. Published studies confirm that volume restoration alone can improve jowls, even without superficial lifting.
The injection planes are supraperiosteal (on the bone), sub-SMAS, and along retaining-ligament insertions. Placing volume at ligament-rich points takes advantage of the tenting effect, where the filler acts like a tent pole that lifts a wider region of overlying tissue.
Masseter Botox and Jowls — Premasseter Space
Patients who have received masseter botox for many cycles sometimes notice that jowls progress more quickly. Above the masseter sits a potential space called premasseter space. While the masseter has full volume this space is collapsed, but when the masseter atrophies after repeated botox, the space expands and the overlying SMAS and buccal fat shift inferiorly — pulling the marionette line and jowls down with them.
This effect is more pronounced in patients over their late thirties with thinned dermis, generous buccal fat, and weak zygomatic support. Using conservative botox doses, anatomically precise placement, and pre-strengthening the dermis and SMAS support are the keys to avoiding acceleration.
Treatment Strategy — HIFU, Collagen Stimulator, Filler
Jowl treatment rarely succeeds as a single modality. A staged combination strategy works best. ① HIFU (Ulthera) re-establishes SMAS-level support. ② Collagen stimulators (Juvelook, Radiesse, Sculptra) thicken the dermis and reinforce the ligament framework. ③ Filler (marionette / mandibular ligament filler) places precise tenting points on the supraperiosteal plane and at ligamentous insertions.
RF (Thermage, Density Alpha-Tip) contributes dermal collagen reinforcement and is often layered in at 6–12-month intervals. The most important step before any of this is precise diagnosis — identifying which of the five layers (bone, deep fat, superficial fat, SMAS, skin) is contributing most determines the order and weight of each modality.
Prevention — Start Cumulative Care from the Mid-Thirties
The first line of prevention is preserving dermal elasticity and accumulating SMAS support. ① Daily broad-spectrum SPF 50+, ② RF and HIFU at 6–12-month intervals from the mid-thirties, ③ collagen boosters to maintain dermal density when indicated, ④ posture (avoiding chronic forward head position) and natural use of facial expression muscles.
Patients on a long-term masseter botox schedule should consider starting with a partial dose for the first cycle to see how their face responds, and combining dermal and SMAS-level support treatments in parallel. Even established jowls can improve substantially with a staged combination plan, so it is rarely too late to start.