Why does melasma respond differently in different patients?
Melasma treatment outcomes vary dramatically between patients because visible appearance doesn't reflect underlying pigment characteristics. Some patients achieve significant clearance with standard therapy while others require 20+ sessions for comparable results, and this difference is entirely predictable if you understand the right factors.
This variation is not coincidental. Melasma that appears identical on the surface may have completely different internal characteristics that dramatically influence treatment response. The most important first step in successful melasma treatment is obtaining an accurate diagnosis of your specific melasma type and characteristics.
Pigment Depth: How Deep Is Your Melasma?
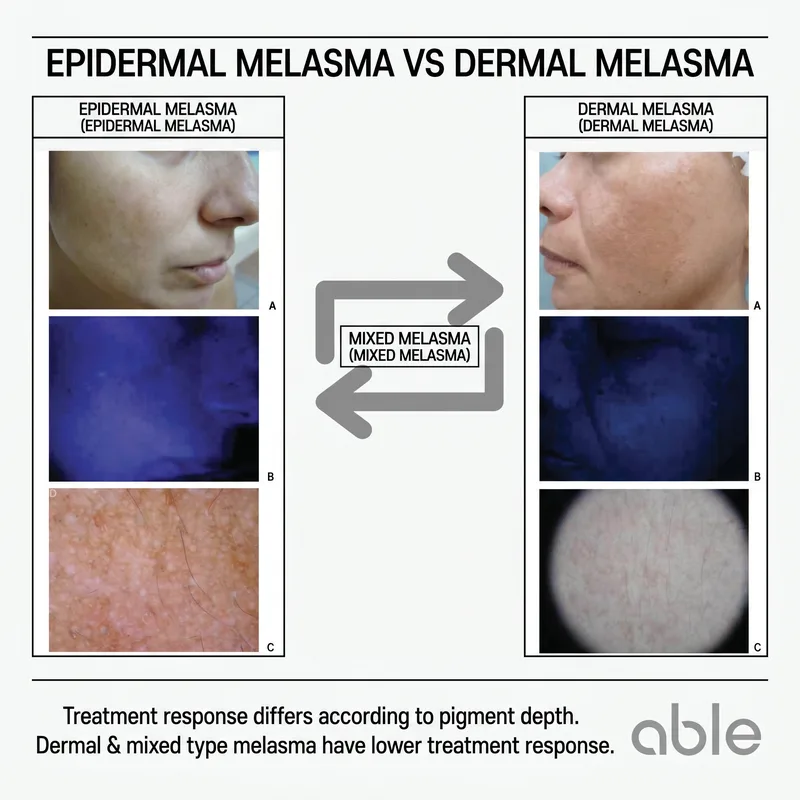
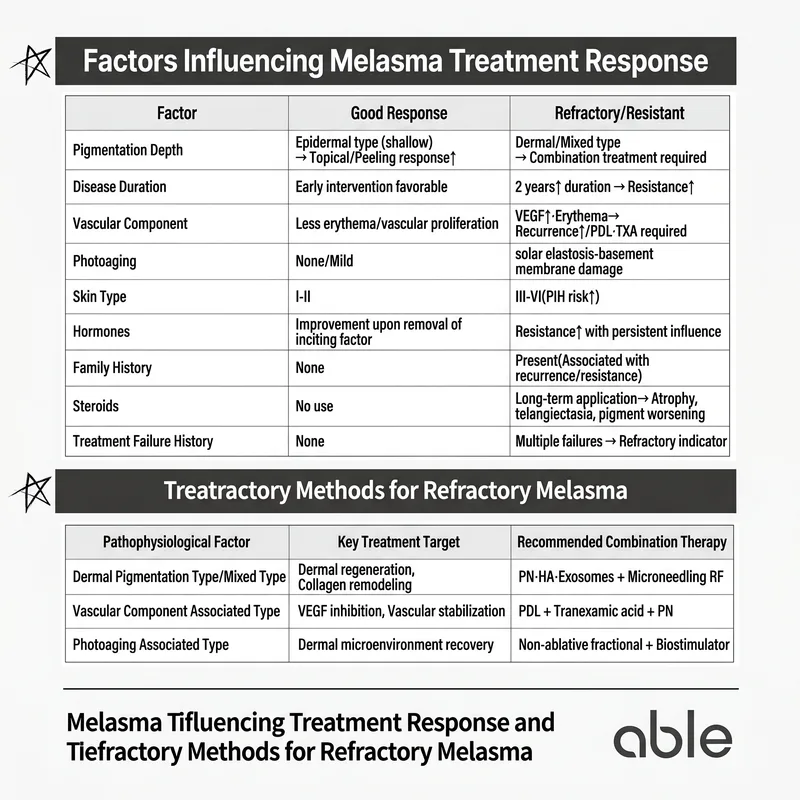
The depth and location of melanin is the single most important factor determining melasma treatment prognosis. Melanin deposits can be located in the epidermis (superficial layer) or dermis (deeper layer), and this depth dramatically affects treatment difficulty.
Epidermal melasma, with pigment located near the skin surface, responds well to treatment. Wood's lamp and dermoscopy clearly reveal the pigment, and appropriate surface-level treatments have excellent improvement potential. In contrast, dermal melasma or mixed epidermal-dermal melasma, where pigment is located deeper, tends to be treatment-resistant. Deep dermal melasma is particularly challenging because melanin is stored in dermal macrophages, making superficial treatments alone ineffective.
Disease Duration: How Long Have You Had Melasma?
Earlier treatment of melasma is significantly more favorable. Melasma persisting for more than two years undergoes structural changes beyond simple melanin accumulation. Long-standing melasma shows dermal degeneration, basement membrane damage, and fibroblast dysfunction. These structural changes mean that melanin removal alone is insufficient; the dermal microenvironment must be restored to prevent recurrence.
Vascular Component: Is Increased Blood Flow Present?
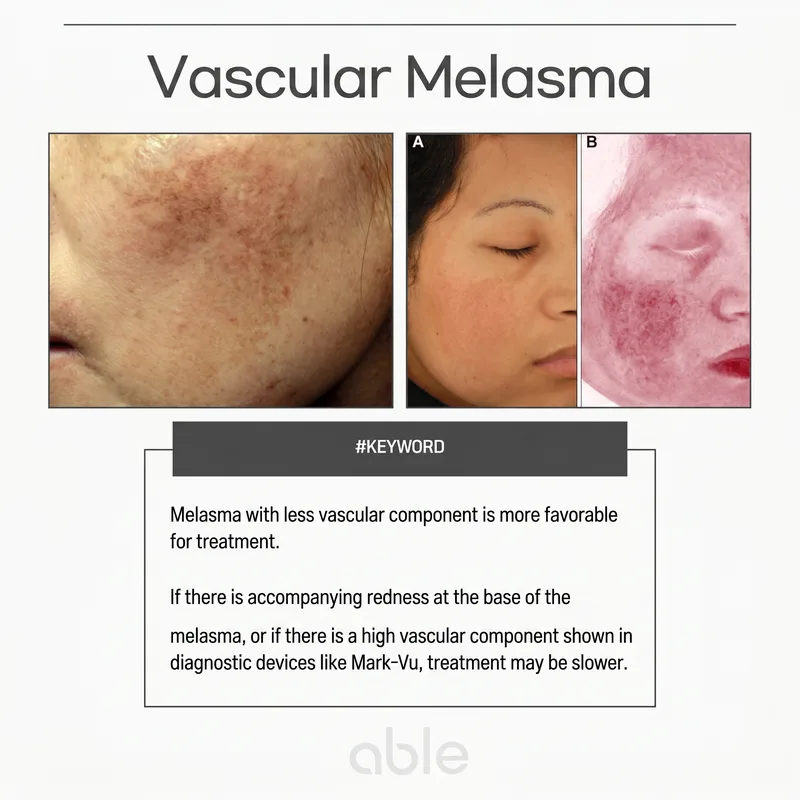
The presence of vascular proliferation within melasma significantly increases treatment difficulty. Melasma with vascular component appears reddish, and blood vessels continuously supply oxygen and growth factors to melanocytes, perpetuating melasma persistence and recurrence. Repeated laser alone may worsen facial redness while the melasma returns.
Melasma with vascular component requires combination treatment: pigment laser plus vascular laser (PDL), supplemented by systemic tranexamic acid to stabilize vascular tone.
Photodamage: How Much Sun Damage Does Your Skin Have?
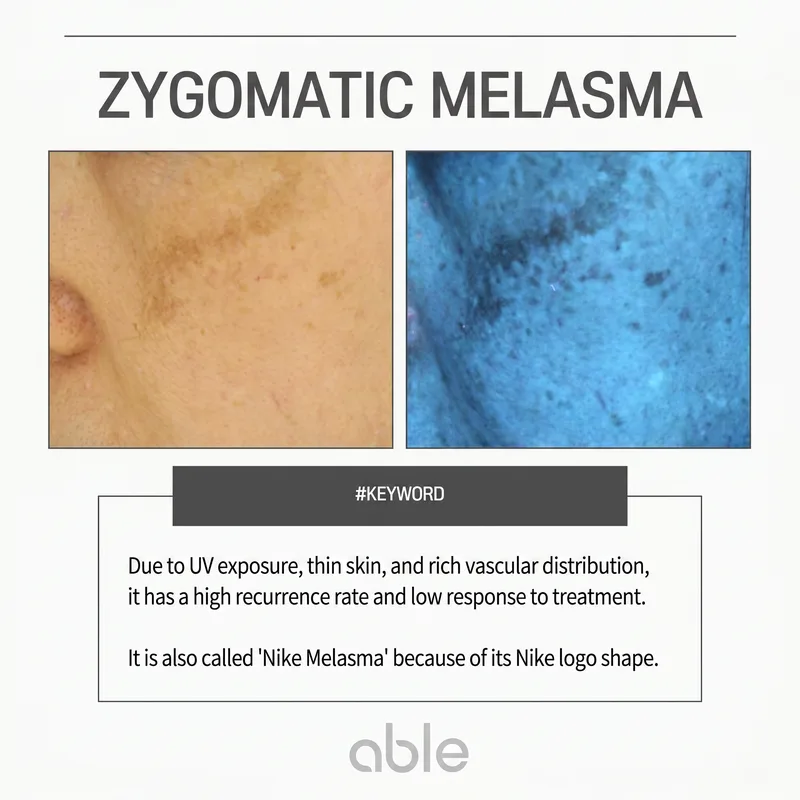
Melasma treatment becomes significantly more complex in chronically photodamaged skin. Chronic sun exposure damages the basement membrane separating epidermis and dermis. When this protective barrier is damaged, a process called melanin incontinence occurs, where epidermal melanin leaks into the dermis. This converts superficial epidermal melasma into deeper dermal or mixed melasma, making treatment far more difficult.
Photodamaged melasma requires pigment treatment combined with dermal regeneration therapies (skinboosters, microneedle RF, fractional laser) to achieve long-term improvement.
Skin Type: Is Your Skin Tone Fair or Deep?
Darker skin types require more conservative melasma treatment approaches. Patients with Fitzpatrick skin types III-VI are at higher risk for post-inflammatory hyperpigmentation if aggressive treatments are applied. Aggressive energy settings used successfully in fair-skinned individuals often backfire in darker skin, worsening pigmentation through treatment-induced inflammation. Fair-skinned patients typically tolerate stronger treatments with fewer side effects.
This is why conservative settings and extended treatment duration are essential for Asian patients with melasma, with the understanding that complete clearance may require significantly longer treatment periods.
Hormonal Factors: Are Hormones Influencing Your Melasma?
Hormones significantly influence melasma treatment response. Hormone-related melasma (from pregnancy, oral contraceptives) shows poorer treatment response and higher recurrence risk because hormones continuously stimulate melanocytes. For patients undergoing hormonal therapy, the realistic first goal is "preventing worsening" rather than "complete clearance," with true cure only possible after hormonal influence ceases (typically after menopause).
Difficult Melasma: A Comprehensive Approach

When multiple unfavorable factors combine—mixed melasma with vascular component, significant photodamage, hormonal influence—simple pigment laser is insufficient. The fundamental principle shifts from "removing melanin" to "restoring the entire skin microenvironment," requiring customized combination therapy addressing three axes: epidermal melanin, dermal fibroblasts, and vascular tone.
Deep dermal or mixed melasma benefits from dermal regeneration with skinboosters (polynucleotides, hyaluronic acid, biostimulators) and microneedle RF combined with pigment laser. Vascular component requires vascular laser (PDL) plus systemic tranexamic acid. Severe photodamage necessitates emphasis on dermal environment restoration and long-term maintenance therapy (antioxidants, hydration, rigorous sun protection).
Melasma Treatment Starts with Accurate Diagnosis
Melasma treatment success depends not on treatment intensity but on diagnostic accuracy and treatment customization. Even identical procedures yield dramatically different results depending on whether the treatment matches your specific melasma characteristics and whether adequate complementary therapies are included.
During your dermatologist consultation, don't stop at a simple "you have melasma" diagnosis. Specifically understand your pigment depth, vascular component status, and degree of photodamage. These determine your treatment plan, duration, and required adjunctive therapies. Melasma never results from a single cause, and individual circumstances always require personalized approaches. Only through accurate diagnosis and comprehensive combination treatment can you minimize recurrence and achieve true skin restoration.
Frequently Asked Questions
- What's the difference between treatable and difficult melasma?
- Epidermal melasma responds relatively well to treatment, while dermal and mixed types are challenging. Six factors determine prognosis: duration, skin type, UV exposure, hormonal status, treatment history, and lifestyle.
- Why is Wood's lamp examination important before melasma treatment?
- Wood's lamp helps determine melasma depth. Epidermal melasma shows enhanced contrast under Wood's lamp, while dermal melasma shows minimal change. This assessment is the first step in treatment planning.
Ready to address your pigmentation concerns?
Pigmentation & Melasma Treatment Schedule a Consultation